
18 May Ebola Bundibugyo Spread in Congo Is a Global Emergency – WHO
This article covers “Daily Current Affairs”
SYLLABUS MAPPING : GS Paper 3 : Environment , Science and Technology
FOR PRELIMS : Ebola Virology , Other Diseases , Vaccines
FOR MAINS : “The repeated emergence of Ebola outbreaks in the DRC — the 17th since 1976, now compounded by spread to Uganda — reveals not just a virological threat but a governance failure: the intersection of state fragility, armed conflict, and inadequate global health financing creates ideal conditions for epidemic emergence.” Critically examine the global governance challenges of containing Ebola outbreaks in conflict zones and the role of international institutions in building more resilient health systems. (15 M)
Why in News?
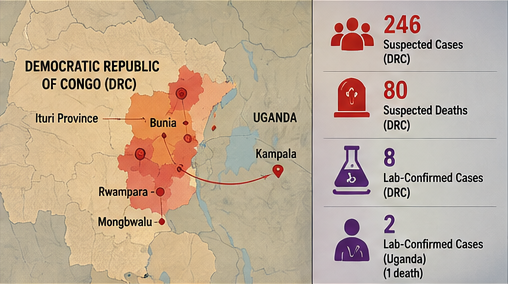
On Sunday, May 17, 2026, WHO Director-General Dr. Tedros Adhanom Ghebreyesus declared the Ebola disease outbreak caused by the Bundibugyo virus in the Democratic Republic of Congo (DRC) and Uganda a Public Health Emergency of International Concern (PHEIC) — the highest alert level in global health governance. As of May 16, 2026, 246 suspected cases and 80 suspected deaths have been reported in Ituri Province, eastern DRC, across at least three health zones — Bunia, Rwampara, and Mongbwalu. Eight laboratory-confirmed cases have been verified. Two additional laboratory-confirmed cases — including one death — have been reported in Kampala, Uganda, among individuals who had travelled from DRC. This is the 17th Ebola outbreak in the DRC since 1976. Critically, unlike the well-known Ebola Zaire strain (for which vaccines like rVSV-ZEBOV/Ervebo exist), the Bundibugyo virus has no approved vaccines or therapeutics globally. In an unprecedented move, Tedros declared the PHEIC without waiting for an Emergency Committee’s recommendation — a first in WHO history — citing the rapidly deteriorating situation.
What Is Ebola? — Virology and Disease Profile
Basic Virology
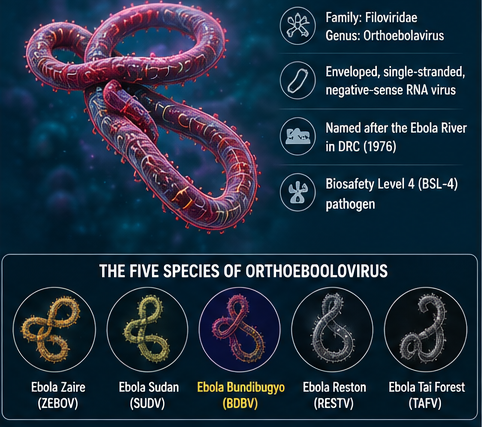
Ebola viruses (genus Orthoebolavirus, family Filoviridae) are among the most feared pathogens on Earth. They are enveloped, single-stranded, negative-sense RNA viruses — the same broad category as measles and influenza, but far more lethal. The name comes from the Ebola River in the DRC (then Zaire), near which the first outbreak was discovered in 1976. The viruses are classified as Biosafety Level 4 (BSL-4) pathogens — the highest risk category — requiring maximum containment laboratories for research.
The Five Species of Orthoebolavirus
| Species (Virus) | First Identified | CFR Range | Vaccine / Treatment? | Note |
|---|---|---|---|---|
| Ebola Zaire (ZEBOV) | 1976, DRC | 25–90% | Yes — rVSV-ZEBOV (Ervebo), rAd26.ZEBOV (Zabdeno-Mvabea) | Most common; caused 2014–16 West Africa epidemic (11,300 deaths); 2018–20 DRC (2,287 deaths) |
| Ebola Sudan (SUDV) | 1976, Sudan | 40–65% | Candidate vaccines in trials (no licensed) | Caused 2022 Uganda outbreak; high CFR |
| Ebola Bundibugyo (BDBV) | 2007, Uganda | 30–50% | No approved vaccine or therapeutic | Current outbreak — 3rd known instance; missed by standard GeneXpert tests |
| Ebola Reston (RESTV) | 1989, Philippines | 0% (human) | Not needed | Non-pathogenic in humans; fatal in non-human primates |
| Ebola Taï Forest (TAFV) | 1994, Côte d’Ivoire | ~0% (single case) | Not applicable | Only 1 confirmed human case; scientist accidentally infected |
How Bundibugyo Differs from Ebola Zaire
No approved vaccine: Unlike Ebola Zaire (which has two WHO-approved vaccines), Bundibugyo has no licensed vaccine or specific antiviral treatment anywhere in the world
Missed by field tests: Standard GeneXpert Ebola tests deployed in field labs only detect Ebola Zaire. The Bundibugyo strain was missed by multiple rounds of field testing — positive cases only confirmed when samples were sent to Kinshasa’s national reference lab (INRB) using multi-species tests
Only 3rd known outbreak: Extremely rare — medical and public health systems have very limited experience with its clinical presentation and outbreak management
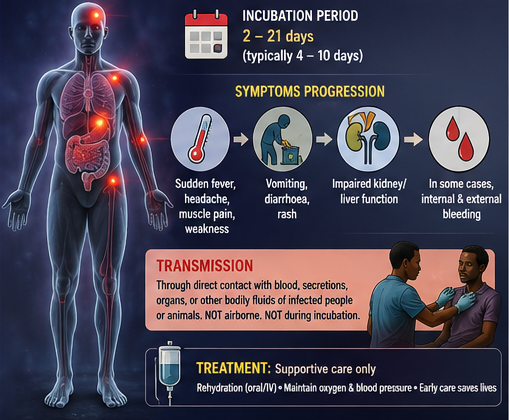
Incubation period: 2–21 days (typically 4–10 days)
Symptoms: Sudden onset of fever, severe headache, muscle pain, weakness → vomiting, diarrhoea, rash → impaired kidney/liver function → in some cases, internal and external bleeding (haemorrhagic fever)
Transmission: Through direct contact with blood, secretions, organs, or other bodily fluids of infected persons or animals; NOT airborne; NOT transmitted during incubation period
Treatment: Supportive care only — rehydration (oral/IV), maintaining oxygen and blood pressure; early care dramatically improves survival
The Outbreak — Full Chronological Timeline
What Is a PHEIC? — IHR Framework Explained
Under Article 12 of the International Health Regulations (IHR) 2005, a PHEIC is defined as “an extraordinary event which is determined to constitute a public health risk to other States through the international spread of disease and to potentially require a coordinated international response.” It is declared by the WHO Director-General after consulting the affected State Parties, and authorises the issuance of Temporary Recommendations to all Member States on travel, trade, and health measures. A PHEIC is the highest alert level in international public health — it explicitly does NOT mean a pandemic (which requires a different set of criteria under IHR 2005 Article 12.2, as revised in 2022 Amendments).

| Feature | PHEIC | Pandemic Emergency |
|---|---|---|
| IHR provision | Article 12(1) — IHR 2005 | Article 12(2) — IHR 2005 (2022 Amendments) |
| Definition | Extraordinary event; international spread risk; coordinated response needed | PHEIC + widespread, accelerating international spread across multiple WHO regions |
| Declared by | WHO Director-General (after consulting affected State Parties) | WHO Director-General (stricter criteria) |
| Emergency Committee needed? | Usually yes — but DG can declare without (as in May 2026 Ebola case) | Yes — Emergency Committee consultation required |
| Border/travel closure? | Advised AGAINST unnecessary restrictions; WHO issues Temporary Recommendations | More extensive international coordination required |
| Current 2026 Ebola status | PHEIC declared — May 17, 2026 | NOT a pandemic emergency — WHO explicitly stated this |
| Previous PHEICs | H1N1 (2009); Polio (2014–present); Ebola West Africa (2014–16); Zika (2016); Ebola DRC (2019); COVID-19 (2020–23); Mpox (2022, 2024) | COVID-19 Pandemic Emergency (under new 2022 criteria — not yet invoked separately) |
Historical Ebola Outbreaks — Key Context
| Year | Location | Virus Strain | Cases | Deaths | Key Significance |
|---|---|---|---|---|---|
| 1976 | DRC + Sudan | Zaire + Sudan | 602 | 431 | First ever identified Ebola outbreaks; named after Ebola River, DRC |
| 2007–08 | Uganda (Bundibugyo) | Bundibugyo | 131 | 42 | First-ever Bundibugyo outbreak; new species identified in Bundibugyo district, Uganda |
| 2012 | DRC (Province Orientale) | Bundibugyo | 57 | 29 | Second Bundibugyo outbreak; CFR ~51%; declared ended December 2012 |
| 2014–16 | West Africa (Guinea, Liberia, Sierra Leone) | Zaire | 28,616 | 11,310 | Largest Ebola epidemic in history; first to cross multiple countries; global health emergency |
| 2018–20 | DRC (North Kivu + Ituri) | Zaire | 3,470 | 2,287 | Second largest; same region as 2026 outbreak; rVSV-ZEBOV vaccine deployed effectively |
| 2022 | Uganda | Sudan | 164 | 77 | No licensed Sudan vaccine; ring vaccination with candidates; outbreak ended Jan 2023 |
| 2025 (Aug–Dec) | DRC (Kasai Province) | Zaire | 64 | 45 | 16th DRC outbreak; ended December 2025 |
| 2026 (May–) | DRC (Ituri) + Uganda | Bundibugyo | 246 suspected + 10 lab-confirmed | 80 suspected | 17th DRC outbreak; 3rd Bundibugyo outbreak ever; PHEIC declared; no vaccine |
Why This Outbreak Is Particularly Alarming — Six Compounding Factors
- No approved vaccine or therapeutic:Unlike Ebola Zaire (two vaccines; monoclonal antibodies Inmazeb and Ebanga), the Bundibugyo strain hasno licensed vaccine, antiviral, or specific treatmentanywhere in the world. Response is limited to supportive care, contact tracing, and barrier nursing
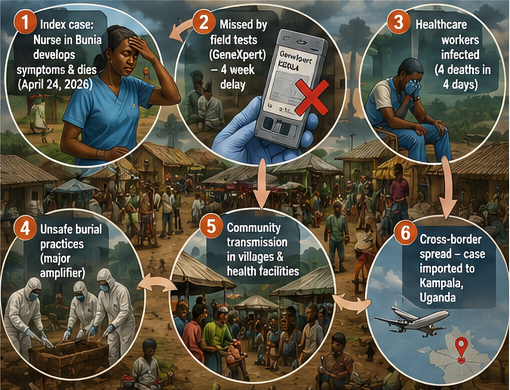
- Missed by standard field tests:GeneXpert tests — the workhorse of Ebola field diagnosis — only detect Ebola Zaire. The4-week gap between symptom onset (April 24) and lab confirmation (May 14)allowed unchecked community transmission; the high positivity rate (8/13 = 62%) suggests the true case count is far larger than reported
- Healthcare worker deaths:Four healthcare workers at Mongbwalu General Referral Hospital died in four days — indicating critical breaches in Infection Prevention and Control (IPC) protocols. Healthcare worker infections historically accelerate any outbreak dramatically
- Ongoing armed conflict in Ituri:Multiple armed groups (including Islamic State-affiliated Allied Democratic Forces and CODECO militia) operate in the mineral-rich Ituri province. Conflict restricts surveillance team movement, limits deployment of Rapid Response Teams, and hinders safe transport of laboratory samples to Kinshasa
- High population mobility and urban spread:Ituri is a commercial and mining hub with a highly mobile population. Bunia — a semi-urban city — is the epicentre. The index case (a nurse in Bunia’s hospital) suggests the virus entered the healthcare system early. Cases have already appeared in Kampala (Uganda) — a capital city of 3.5 million — through travel
- Unsafe burial practices:A large number of community deaths associated with traditional burial practices — involving direct contact with the deceased’s body — are a major amplification mechanism, as Ebola bodies remain infectious after death.
India’s Relevance — Exposure, Preparedness, and IHR Obligations
While India has never experienced a confirmed Ebola outbreak, this PHEIC declaration has significant implications for India’s public health preparedness systems, IHR obligations, and global health engagement.
- IHR Focal Point obligations: As a WHO member state, India’s National IHR Focal Point (under the Ministry of Health & Family Welfare) is obligated to put port-of-entry health screening on heightened alert — particularly for travellers arriving from DRC, Uganda, and transit countries in East Africa
- Indian diaspora in East Africa: A significant Indian-origin community lives in Uganda, Kenya, and Tanzania. The DRC itself has Indian health workers and NGO staff operating in conflict zones
- IDSP and NCDC: India’s Integrated Disease Surveillance Programme (IDSP) and the National Centre for Disease Control (NCDC) are activated to monitor any imported cases; all international travellers from affected regions are subject to health declaration at entry points
- BSL-4 capability gap: India currently has only one BSL-4 laboratory — at the National Institute of Virology (NIV), Pune. Bundibugyo virus, as a BSL-4 pathogen, requires this maximum-containment facility for any diagnostic work; sample collection protocols are in place
- Vaccine manufacturing role: India as the “pharmacy of the world” has a potential future role in manufacturing any Bundibugyo vaccine candidate once one is approved; COVAXIN manufacturer Bharat Biotech and Serum Institute of India have previously expressed interest in Ebola vaccine manufacturing
- One Health framework: The outbreak’s likely zoonotic origin (Ebola is thought to be harboured in fruit bats) reinforces India’s commitment to a One Health approach — integrating human, animal, and environmental health surveillance — under the National One Health Mission
Practice Questions
1. The Bundibugyo virus belongs to the genus Orthoebolavirus, and the 2026 outbreak in the DRC and Uganda is the third documented outbreak of this specific Ebola species, with the first having occurred in Uganda in 2007–08.
2. Unlike the Ebola Zaire strain, for which WHO-approved vaccines such as rVSV-ZEBOV (Ervebo) exist, there are currently no approved vaccines or specific therapeutics for the Bundibugyo strain of the Ebola virus.
3. A Public Health Emergency of International Concern (PHEIC) declared under the International Health Regulations (IHR) 2005 automatically mandates WHO member states to close their international borders and halt all air travel to and from the affected countries.
4. The 2026 Bundibugyo outbreak was the first instance in WHO history where a PHEIC was declared without a prior recommendation from an Emergency Committee.
Which of the statements given above are correct?
Statement 1 is CORRECT. The Bundibugyo virus (BDBV) is one of five species in the genus Orthoebolavirus (family Filoviridae). The first documented Bundibugyo outbreak occurred in 2007–08 in Bundibugyo district, western Uganda, with 131 cases and 42 deaths — and the virus was named after that location. The second outbreak was in the DRC’s Province Orientale in 2012, with 57 cases and 29 deaths. The 2026 DRC-Uganda outbreak is therefore the third documented Bundibugyo outbreak in recorded history, making it an exceptionally rare event with very limited prior public health response experience.
Statement 2 is CORRECT. The WHO has approved two vaccines for Ebola Zaire: rVSV-ZEBOV (brand name Ervebo, manufactured by Merck) and a two-dose regimen of rAd26.ZEBOV + MVA-BN-Filo (brand names Zabdeno and Mvabea, manufactured by Johnson & Johnson). Additionally, two monoclonal antibody treatments — Inmazeb and Ebanga — are approved for Ebola Zaire. However, for the Bundibugyo strain, no vaccine, antiviral, or specific therapeutic is licensed anywhere in the world. Response must rely entirely on supportive care, IPC, and contact tracing — which is why the 2026 outbreak carries exceptional risk.
Statement 3 is INCORRECT. A PHEIC under IHR 2005 does NOT automatically mandate border closures or suspension of air travel. In fact, IHR 2005 explicitly states that WHO should advise AGAINST unnecessary travel restrictions and border closures, as these can disrupt the international response and drive outbreak information underground. What a PHEIC does is: authorise the WHO Director-General to issue Temporary Recommendations (guidance on health measures at borders, ports, and airports); elevate political and financial attention to the outbreak; and establish a framework for coordinated international response. Border closures are a unilateral decision of individual member states, not a mandatory consequence of PHEIC declaration.
Statement 4 is CORRECT. The May 17, 2026 PHEIC declaration for the Ebola Bundibugyo outbreak was the first time in WHO history that a PHEIC was declared without waiting for a recommendation from an Emergency Committee. WHO Director-General Tedros Adhanom Ghebreyesus cited the rapidly deteriorating situation — the high sample positivity rate, four-week detection gap, healthcare worker deaths, community deaths, conflict in Ituri, and Kampala cases — as justification for acting without waiting for the committee’s formal recommendation. He did, however, state that an Emergency Committee would be convened “as soon as possible” to issue formal Temporary Recommendations.
Mains Questions
- Why Are Government Schools Shutting Down? - August 3, 2026
- Analysing the Supreme Court’s Judgment on Sex Work - August 3, 2026
- Strong Health Systems for All with Better Public Spending - August 3, 2026

No Comments